
Content created by Assistant Secretary for Legislation (ASL)
on
Investing in Native Communities: Transformative Opportunities in the Infrastructure Investment and Jobs Act
before
Field Hearing of the Senate Committee on Indian Affairs
Good morning Senator Smith and Members of the Committee. Thank you for the opportunity to provide another update on Indian Health Service (IHS) programs benefitting American Indian and Alaska Native communities under the Infrastructure Investment and Jobs Act (IIJA).
The IHS is an agency within the Department of Health and Human Services (HHS) and our mission is to raise the physical, mental, social, and spiritual health of American Indians and Alaska Natives to the highest level. This mission is carried out in partnership with American Indian and Alaska Native Tribal communities through a network of over 687 Federal and Tribal health facilities and 41 Urban Indian Organizations (UIOs) that are located across 37 states and provide health care services to approximately 2.7 million American Indian and Alaska Native people annually.
Sanitation Facilities Construction Program
The 1988 amendments to the Indian Health Care Improvement Act require IHS to maintain inventories of sanitation deficiencies for existing Indian homes and communities, to prioritize those deficiencies, and to annually report those deficiencies to Congress. Since 1989, IHS has annually reported these needs to Congress in the form of projects, which are currently catalogued in the Sanitation Deficiency System (SDS). Projects are identified in terms of the facilities to be provided, the cost of those facilities, and the number of homes to be served by the facilities. Funding for projects is distributed to the Areas based on an allocation formula that takes into account the relative needs identified in each Area’s SDS inventory. The Sanitation Facilities Construction (SFC) program employs a cooperative approach for planning, designing and constructing sanitation facilities serving American Indian and Alaska Native communities. Each project is initiated at the request of a Tribe or Tribal Organization, and coordination is maintained throughout project planning, design and construction.
At the end of fiscal year (FY) 2021 about 7,228, or 1.9 percent of all American Indian and Alaska Native homes tracked by IHS lacked water supply or wastewater disposal facilities; and, about 108,459 or approximately 29 percent of American Indian and Alaska Native homes tracked by IHS were in need of some form of sanitation facilities improvements. Many of these homes without service are typically located in remote locations such as on the Navajo Nation and in some remote Alaska Native Villages. The capital cost to construct these facilities are significantly higher than the provision of similar facilities in other geographic locations. Additionally, the cost burden associated with operation and maintenance of these facilities usually exceeds the capacity of the Tribal utility to generate sufficient revenue from the system users to support ongoing operation.
The IHS tracks sanitation projects in the SDS. The list of sanitation projects in the SDS is not static. In collaboration with Tribes, IHS annually updates the SDS project listing to account for the addition of newly identified sanitation deficiencies and to update cost estimates due to increases related to inflation, labor and material costs, and project scope changes.
At the end of FY 2021, the SDS included 1,513 projects. Of this total, 945 projects were feasible and 568 projects were infeasible with a combined total database cost estimated at $3.4 billion in eligible costs and an additional $735 million in ineligible costs that will have to come from other non-IHS funding resources.
Ineligible costs are the costs associated with serving commercial, industrial, or agricultural establishments, including nursing homes, health clinics, schools, hospitals, hospital quarters, and non-American Indian and Alaska Native homes. The Sanitation Facilities Construction Act prevents the IHS from using its appropriations for these costs. However, the IHS regularly partners with Tribes and other Federal Agencies to identify alternative resources to successfully support these ineligible costs. If our Federal funding partners are not able to contribute financial support for the projects that have IHS ineligible costs, those projects will not be fully funded and hence cannot be completed if the Tribe does not have the financial capability to fund the ineligible portion of the project.
Economically infeasible projects are those that exceed a per unit cost set for each IHS Area, and three different regions within the IHS Alaska Area. While there was not a statutory barrier to funding economically infeasible projects, the IHS had not been able to fund these projects in light of limited annual appropriations before the IIJA was enacted. The IIJA provided $2.2 billion for economically infeasible projects.
The IHS categorizes SDS projects into three Tiers depending on a project’s progress toward completing planning activities.
- Tier 1 projects are considered ready to fund because planning is complete. However, design and construction contract document creation activities are not yet complete for current Tier 1 projects. These projects then move through the design and construction contract document creation steps before a construction contract can be initiated through Federal or Tribal procurement methods.
- Tier 2 projects are projects that have a level of engineering assessment completed, such that the deficiency is understood and a recommended solution has been analyzed and scoped; these projects have a cost estimate and design parameters that are accurate within plus or minus 25 percent.
- Tier 3 projects are projects with cost estimates and design parameters that do not have a specific accuracy target, but are based on the best information available at the time of submission. These projects demonstrate that an eligible deficiency has been identified, but the Area may not have determined the recommended solution.
The IHS also assigns a Deficiency Level to each project in the SDS. Deficiency Levels are assigned in accordance with section 302(g)(4) of the Indian Health Care Improvement Act (IHCIA) (25 U.S.C. § 1632(g)(4)) for each sanitation facilities project that has been identified as a need to support Indian Tribes and communities. The Deficiency Levels are explained in the table below.
| Sanitation Deficiency Level | Description |
|---|---|
| V | An Indian tribe or community that lacks a safe water supply and a sewage disposal system. |
| IV | An Indian tribe or community with a sanitation system which lacks either a safe water supply system or a sewage disposal system. |
| III | An Indian tribe or community with a sanitation system which has an inadequate or partial water supply and a sewage disposal facility that does not comply with applicable water supply and pollution control laws, or has no solid waste disposal facility. |
| II | An Indian tribe or community with a sanitation system which complies with all applicable water supply and pollution control laws, and in which the deficiencies relate to capital improvements that are necessary to improve the facilities in order to meet the needs of such tribe or community for domestic sanitation facilities. |
| I | An Indian tribe or community with a sanitation system which complies with all applicable water supply and pollution control laws, and in which the deficiencies relate to routine replacement, repair, or maintenance needs. |
| 0 | No deficiencies to correct. |
SFC projects can be directly operated by the IHS through Federal Acquisition Regulation contracts or through Tribal procurement. Tribes can directly operate SFC projects through Indian Self-Determination and Education Assistance Act construction contracts (25 C.F.R. 900 Subpart J, 42 C.F.R. 137 Subpart N).
Infrastructure Investment and Jobs Act
The IIJA appropriated a total of $3.5 billion to the IHS SFC program. The Act includes $700 million annually from FY 2022 through FY 2026. The Act includes a maximum 3 percent ($21 million) set-aside for salaries, expenses, and administration each year. These funds are limited to Federal costs only. It also directs that the IHS provide 0.5 percent ($3.5 million) each year to the Office of Inspector General for oversight of these funds. Finally, the Act also directs the Agency to use up to $2.2 billion of the $3.5 billion appropriation on economically infeasible projects.
The IIJA funds will support the construction of water, wastewater, and solid waste facilities in American Indian and Alaska Native tribes and communities. The IHS support for these facilities is an integral component of IHS disease prevention activities. As a result, infant mortality rates and mortality rates for gastroenteritis and other environmentally-related diseases have declined. Research supported by the Centers for Disease Control and Prevention states populations in regions with a lower proportion of homes with water service, reflect significantly higher hospitalization rates for pneumonia, influenza, and respiratory syncytial virus.1 Researchers associated the increasing illnesses with the restricted access to clean water for hand washing and hygiene.
The SFC Program works collaboratively with Tribes to assure all American Indian and Alaska Native homes and communities are provided with safe and adequate water supply and waste disposal facilities. The residents of these homes will benefit from reduced health care cost associated with water related illnesses. The IHS estimated in FY 2021 that for every $1 in funding provided for sanitation facilities resulted in $1.23 in avoided medical cost related to inpatient and outpatient visits related to respiratory, skin and soft tissue, and gastro enteric disease. As required by the bill, IHS will update the Congressional spend plan for these funds annually through FY 2026.
FY 2022 Infrastructure Investment and Jobs Act Funding Allocations
On May 31, 2022, the IHS announced the FY 2022 allocation decisions for $700 million appropriated to the IHS in the IIJA.
The IHS conducted 3 virtual tribal consultations on the IIJA from November 22, 2021, to January 5, 2022, and based on review and consideration of input received through tribal consultation, the IHS decided to use current Sanitation Deficiency System data and the agency’s existing funding mechanisms to allocate these resources. This includes IHS direct service projects funded through Federal Acquisition Regulations contracts or tribal procurement, and Indian Self-Determination and Education Assistance Act construction contracts.
The IHS will allocate approximately $581 million in FY 2022 IIJA funding for Tier 1 project construction costs. A Tier 1 project is considered ready to fund because planning is complete. The IHS will also allocate $60 million for design and construction document creation activities related to these Tier 1 projects, which include engineering design activities for proposed sanitation facilities, contract documents, and contract plans and specifications.
Tier 2 projects have a level of their engineering assessment complete and have a well understood deficiency and a recommended solution while Tier 3 projects have deficiencies identified but are still in the planning phase, which may include identifying solutions. The IHS will allocate approximately $33 million in FY 2022 IIJA funding for the planning, design, and construction contract document creation for Tier 2 and Tier 3 projects. The IHS will also use FY 2022 annual appropriations to support additional planning, design, and construction document creation activities for Tier 2 and Tier 3 projects. The SDS currently includes 661 Tier 2 projects, totaling approximately $2.2 billion, and 361 Tier 3 projects, totaling approximately $505 million.
These allocation decisions align with recommendations from tribal leaders to prioritize funding for projects that have completed the planning phase and can be immediately placed into the design and construction phase, and to provide sufficient funding for planning and design activities to get projects ready to fund.
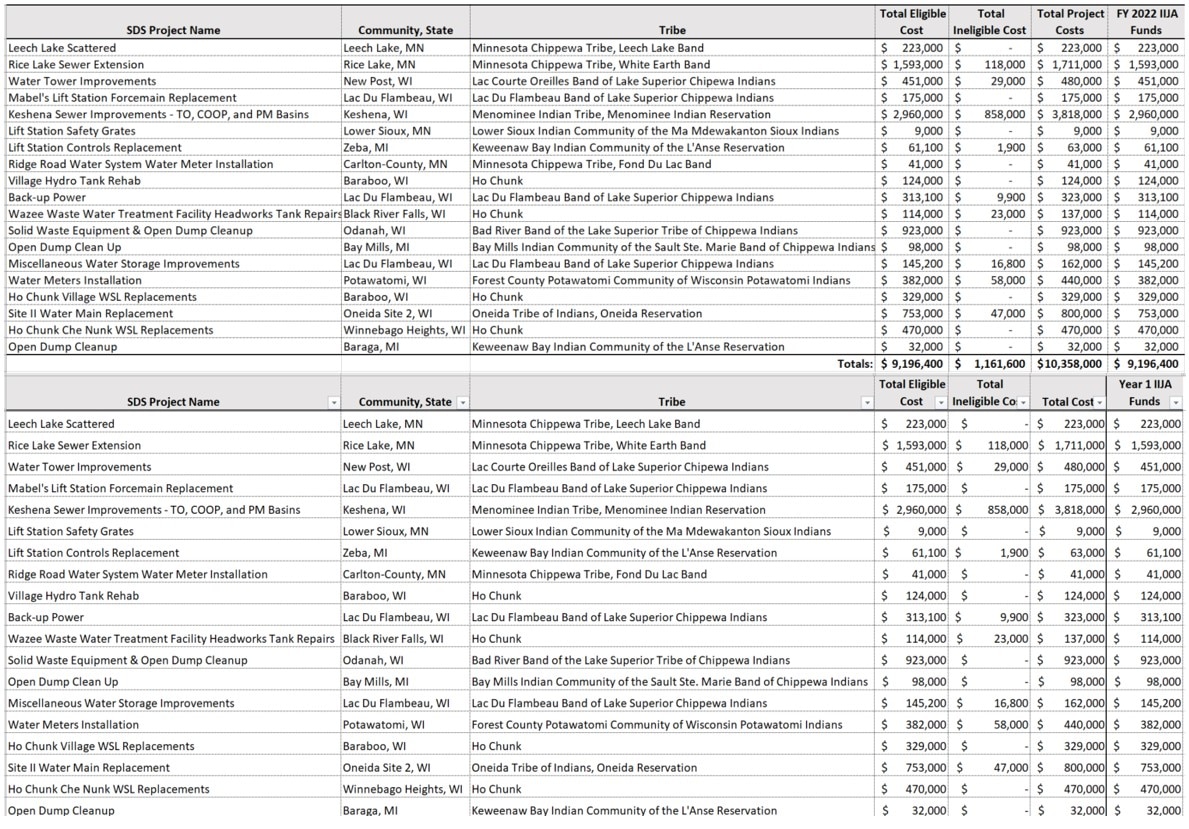
Within the IHS Bemidji Area, 19 Tier 1 projects totaling nearly $9.3 million in IHS eligible costs will be fully funded with the IIJA FY 2022 appropriation. A listing of the Bemidji Area Tier 1 projects is provided below:
Sanitation Facilities Construction Workforce and Support Resources
Historically, IHS has received limited program support resources to address the SFC project workload. SFC project funding has increased since FY 2018, and the IIJA funding will significantly increase the SFC workload. However, the IIJA limits funding for program support activities to 3 percent per year. Given this limitation, it is possible that the average project duration could be greater than the current average project duration of 3.6 years. The IIJA also restricts program support funding to federal activities, which means that Tribes that operate their SFC projects directly cannot access these needed administrative resources.
To address this need for administrative support, the FY 2023 President’s Budget requests +$49 million in Facilities and Environmental Health Support resources to support IIJA implementation. This funding would be available for federal activities and to Tribes who compact or contract under the Indian Self-Determination and Education Assistance Act to implement SFC projects, unlike the administrative set-aside in the IIJA. This investment is critically necessary to maintain existing project completion deadlines and ensure successful implementation of IIJA resources.
The IHS will leverage the use of multiple strategies and available authorities to support IIJA recruitment and hiring, including the use of global and open-ended job announcements to streamline the hiring of multiple candidates for jobs across the IHS system, developing a dedicated website to focus on the recruitment of these positions, and targeting job fairs. The IHS will also explore compensation flexibilities, like special salary rates and authority to approve larger recruitment, relocation, and retention incentives. Such incentives are necessary to increase IHS’ competitiveness with both private and public sector organizations.
We look forward to continuing our work with Congress related to the SFC program and the use of IIJA funds to make improvements in tribal communities. We are committed to working closely with our stakeholders and we understand the importance of working with partners to address the needs of American Indians and Alaska Natives.
Endnotes
1 Thomas W. Hennessy, Troy Ritter, Robert C. Holman, Dana L. Bruden, Krista L. Yorita, Lisa Bulkow, James E. Cheek, Rosalyn J. Singleton, and Jeff Smith. The Relationship Between In-Home Water Service and the Risk of Respiratory Tract, Skin, and Gastrointestinal Tract Infections Among Rural Alaska Natives. American Journal of Public Health: November 2008, Vol. 98, No. 11, pp. 2072-2078.